
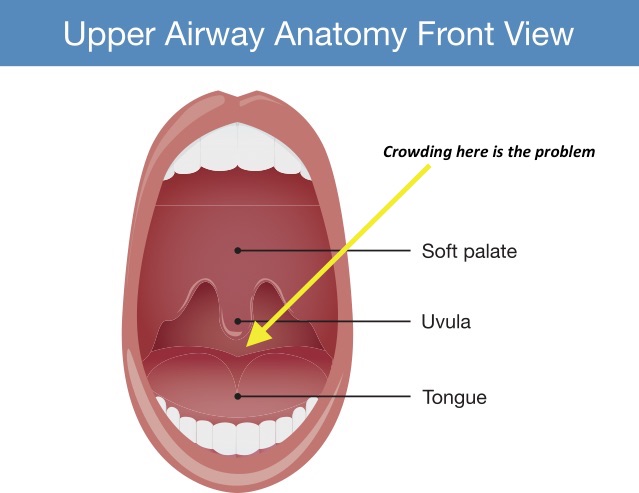
In OSA, when our muscles relax in sleep there is collapse of the back of the throat due our big tongues and floppy muscles. If the collapse is very mild then snoring will occur from vibration of the tissues. If more significant obstruction occurs, air cannot pass down into the lungs causing blood oxygen levels to fall. The fall in blood oxygen is detected by our brains, causing us to be woken briefly from sleep, and a temporary surge in adrenaline. As we wake, tone is put back into our tongue and flopping muscles, opening the airway and allowing oxygen to get down into the lungs. But as we drift off to sleep the process occurs over and over again. Sleep is unrefreshing as our brains are being woken and our health suffers as a result of the poor quality sleep and adrenaline surges.

Obstructive sleep apnoea is really very common. In the USA it is estimated at 6% of the adult population has sleep apnoea. Australian data estimates there are more than 774,590 people living with OSA and that number is increasing every year.
The only way to diagnose OSA is with a diagnostic sleep study. This is important to be done properly to grade the severity of OSA and the position in which it occurs. The severity of OSA is graded by the number of times breathing is interrupted per hour.
- Normal sleep – fewer than five interruptions per hour
- Mild sleep apnoea – between 5 and 15 interruptions per hour
- Moderate sleep apnoea – between 15 and 30 interruptions per hour
- Severe sleep apnoea – more than 30 interruptions per hour.
The symptoms of OSA are variable but include
- Unrefreshing sleep
- Waking with morning headache
- Waking through the night with snoring, gasping or chocking
- Sleepiness during the day